 What we see is a new type of war veteran, the international humanitarian worker, returning from the battlefields unable to escape the horrors there. It is obviously very important that aid organisations begin considering seriously the factors affecting their project personnel. Someone must be able to spot the danger signals at an early stage, and help exposed personnel in dealing with their situation (Smith et al, 1996).
Relief workers today are faced with situations which generate more stress than straightforward natural disasters. This happens in a context in which the usual support mechanisms of family, partner or close friends are absent. Furthermore, the culture in the humanitarian community, which may be one of bravado and competition in emergency situations, does often not allow the space for discussing issues such as psychological stress. Despite mounting anecdotal evidence that stress and its consequences are key occupational health hazards, humanitarian agencies have not moved quickly enough to minimise the risks to the psychological well-being of their staff,. Some common problems Some of the common stress-related problems seen in relief workers include burnout, psychosomatic disorders, and risk-taking behaviour such as alcohol abuse. Unlike domestic rescue workers who are periodically exposed to short stressful events, relief workers may suffer exposure to chronic low levels of stress by, for example, residing in insecure environments for many years. It is in this setting that stress may be cumulative. Burnout is probably the most commonly used lay term associated with cumulative stress. It is a process that is usually gradual in onset. Symptoms can be grouped into five categories (Kahill, 1988):
Acute stress disorder (ASD) and post-traumatic stress disorder (PTSD) are more formal diagnoses related to exposure to severe traumatic stressors such as a direct assault or abduction (primary traumatisation) or witnessing the death or abduction of a colleague (secondary traumatisation). The phenomenon of tertiary traumatisation is also increasingly recognised (Jensen, 1999). Examples include being witness to mass violence or listening to first-hand accounts of traumatised people. ASD appears relatively quickly after exposure to a particular stressor and, by definition, resolves within a month. It includes a spectrum of emotional reactions, cognitive changes such as confusion, and symptoms of mental and physical hyperactivity. PTSD symptoms appear from one month to three months after a given event. Symptoms usually involve flashbacks to the events and a state of being hyper-alert. Symptoms may become chronic and extremely debilitating. In their attempt to find a new internal equilibrium, relief workers may also respond to unresolved stress with more subtle behavioural changes. One such reaction has been termed “enmeshment” and is akin to survivor guilt with an over identification with the beneficiary population (Smith et al, 1996). This reaction may be more common in the younger, more idealistic relief worker. By contrast, avoidance reactions of distancing, withdrawal and denial may be more common among experienced personnel. Finally, relief workers may exhibit self-destructive behaviours such as working to the point of exhaustion, consuming excessive amounts of alcohol, or engaging in unprotected sexual encounters. Problems exacerbated by the humanitarian sector Many of these problems may be exacerbated by factors particular to the humanitarian sector. For example, relief workers do not usually benefit from being in a well-trained, tightly knit unit with a clear command structure. In addition, training and briefing, particularly with regard to psychological issues, is generally inadequate. This is particularly pertinent for those organisations which deploy a high proportion of first assignment volunteers. Third, aid workers are often called upon to perform duties outside their realm of professional competency and experience. Finally, there is the pressure when the drive to ensure the visibility of their own organisation may over-ride questions of the appropriateness or quality of interventions. Two other issues deserve mention because they are relatively modern sources of tension in the humanitarian sector. First, is the pressure of discovering that one’s internal mandate in terms of personal ethics and preferred approach does not match the mandate of a particular organisation. Second, is the changing culture of humanitarian work. Organisations are more self-critical than previously and are increasingly putting resources towards evaluating their activities. Inevitably external criticism, even if constructive, leads to a re-assessment of an individual’s perception of his/her own effectiveness. The latter is particularly true if individuals have an unrealistic expectation of what they may achieve under any given circumstance. Recommendations An individual has three levels of resources, personal, social and organisational, at his/her disposal with which to tackle demands. Organisations should seek to strengthen these resources wherever possible. The personal level: Selection and training are key areas where organisations could better support their personnel. In the past the key qualities organisations have looked for when selecting personnel are flexibility, maturity, adaptability, ability to work in a team and past experience in emergency situations (McCall & Salama, 1999). While experience is crucial, this must be tempered by the knowledge that stress can be cumulative, especially in the setting of aid workers going directly from one emergency to the next. Individuals who have a past psychiatric history including that of alcohol abuse or those with a recent significant life event such as a relationship break up should be regarded as being at higher risk of psychological distress. More effort needs to be made to ensure that an individual understands and is comfortable with the mandate of the organisation and has a realistic expectation of living conditions, security conditions, potential risks including to psychological health and what can be achieved in the circumstances. Some examples of best practice in this setting include being interviewed by the person directly responsible for the project by telephone or in person, and in-depth discussion of hypothetical field scenarios that illustrate some of the complex trade-offs inherent in humanitarian work. Studies in various settings have shown that untrained, poorly briefed staff suffer most from stress-related illness (Ursano & McCarroll, 1994). Briefing and debriefing should be mandatory and in person. It should cover an individual’s personal and emotional reaction to their work environment, not merely the programmatic or administrative issues encountered. A briefing and debriefing by a psychotherapist should represent the standard for all emergency assignments. Mental health professionals working in this role should themselves ideally have experience of humanitarian emergencies. Training courses should cover stress management techniques (types of stress, coping strategies, how to access help within the organisation), cross-cultural issues, team building/conflict resolution strategies, as well as the ethical frameworks and moral dilemmas of humanitarian relief. Courses should also help to prepare recruits for the task of adapting their professional skills to an environment which may demand a very different orientation. The social level: Organisations should be more willing to accommodate couples on assignment, particularly if both have relevant skills. Unless situations pose extreme risk, couples themselves should be given the autonomy to weigh the benefits and risks of the presence of an accompanying partner. Managers should consider flexibility in breaks so as to maximise, wherever possible, couples’ time together. It is also important that those responsible for recruiting understand the team dynamic in each particular field and attempt to match new recruits to a field that will potentially suit them. The organisational level: Formal policies on the prevention of stress in the humanitarian sector are frequently non-existent or incomplete and vary significantly from one organisation to the next (McCall & Salama, 1999). Strategies for improving briefing, training and debriefing need to take place in the context of organisations developing clear, written and comprehensive policies on the psychological health of their employees. Within the framework of institutional policies, mechanisms to support relief workers in the field need more detailed elaboration. A formal mentoring system for new personnel or the designation of a particular individual chosen by his peers in the field to act as the support person for that particular area are two examples of current practice. Policies on the use of critical incident stress debriefing (CISD) also need to be put in place. CISD may be a useful technique particularly in acutely traumatic events such as a line-of-duty death. Furthermore, organisations should come to a consensus on the most appropriate methods for psycho-social follow-up of employees so that they are able to determine what happens to their workers after leaving the organisation; the success with which they negotiate the difficult transition back into their former environments, as well as the proportion that suffer psychological distress. Anonymous cross-sectional surveys at regular intervals are one possibility. Finally, there must be a recognition of the effects on empathetic field managers of coping with the stress of numerous employees. In effect this is a form of tertiary traumatisation and they too must be able to recognise the symptoms of stress in themselves and call in re-enforcements if necessary. Peer support networks of regional managers often occur on an ad hoc basis but this could be made more formal. Conclusion Unfortunately, humanitarian emergencies are becoming more common. Concurrently the humanitarian sector is becoming larger and more professional, and we are seeing a new type of professional: the career relief worker. These environments, however, are not ordinary work places; they expose individuals and organisations to new dilemmas and new challenges. Staff turnover is high and burnout is common. Perhaps the crucial element in the achievement of the humanitarian goal today is the development of a stable and experienced workforce whose energies are effectively harnessed through more enlightened organisational policies. When seen in this light, the psychological support of relief workers is simply part of the employer’s duty and responsibility. It is not an optional extra.
0 Comments
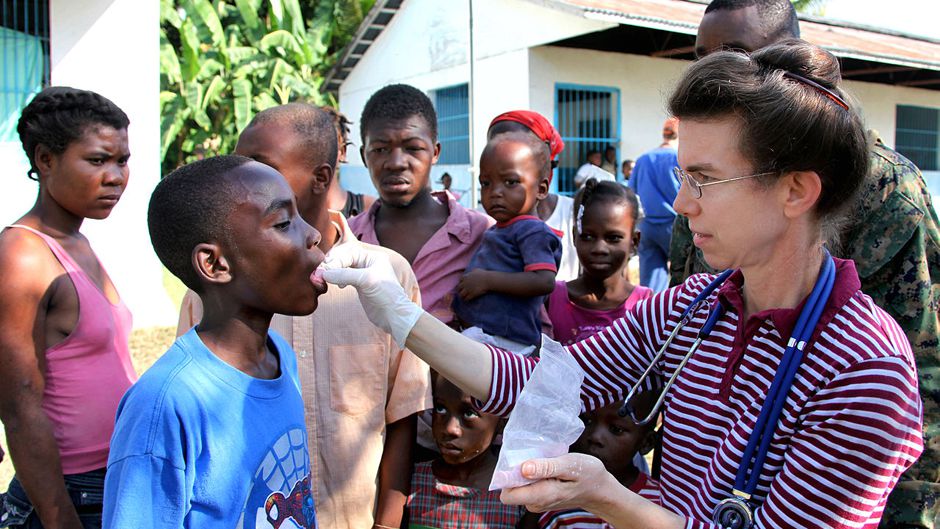
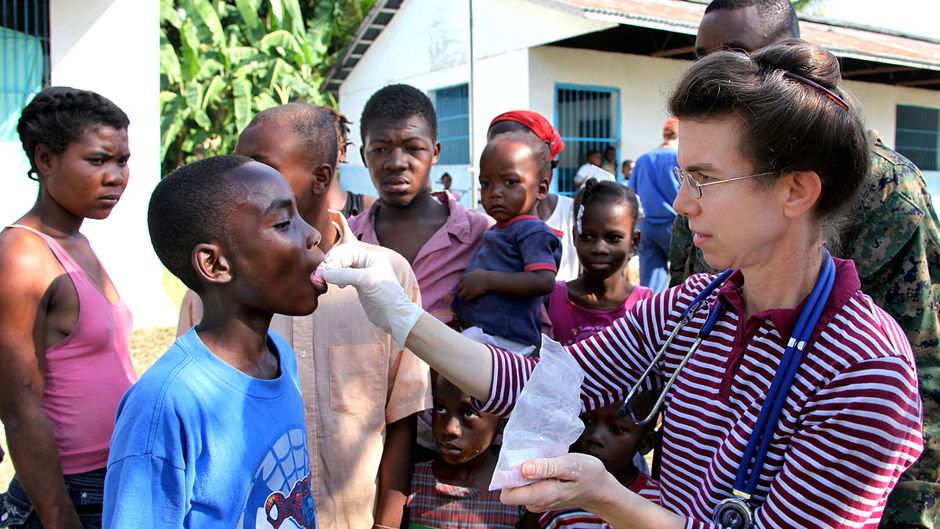 Humanitarian aid workers are routinely exposed to traumatic events linked to the cause of mental health issues including depression, burnout and anxiety. But increasingly, work stress including extremely heavy workloads, long hours and limited time for self-care are being highlighted as major causes. Among volunteers, mental health issues can be even higher. Often from affected communities, volunteers experience the same loss and grief as those they are working to support but without the same training, support or structure as professional workers.
At the global level, there is now increasing recognition of the importance of ensuring the well-being and safety of humanitarian workers and volunteers. However, too often the appropriate support and care systems are not in place, especially for national or local staff. A recent study found that only 20% of aid workers surveyed felt adequate psychosocial support was being offered (Dunkley, 2018). The prevailing culture of silence, feelings of guilt and perceived stigma around mental health, leads many to continue working without seeking treatment. To reduce stress, burnout and to promote the well-being of workers and volunteers, simple and cost-effective initiatives can be put in place before, during and after deployment. Where are we going wrong? Dr Idit Albert, a clinical psychologist specialising in anxiety disorders and trauma, believes that one of the problems is the stigma of mental health in this sector. She points out that, “you wouldn’t send firemen into a fire without the right equipment or training, it’s like in any other profession of care; we’re not talking about providing people with lavish lifestyles but what they need to be able to carry out their work, cope with the situations and be able to resume their lives when they return home.” The problem it seems in the humanitarian sector is the difficulty of transforming that raw compassion into the practical skills necessary, which in turn puts those who may not be fully prepared in a vulnerable situation. The culture of silence Despite NGOs recognising the mental health issues plaguing humanitarian workers, speaking up can sometimes be hard. Self-care is a very easy to say, but very hard in practice. Michael McHugh, a nurse and child protection officer who was one of the first to volunteer in the camps in Calais, feels his training as a nurse gave him those “professional boundaries” necessary that some younger volunteers without training couldn’t seem to grasp, from fear of not being a “true humanitarian”. Mandatory breaks became an actual thing. People were struggling to look after themselves because their focus was outwards, but when people burnout, they can become destructive, which can affect those in their care. This feeling of compassion is what drives aid workers and volunteers, but if the worker becomes unbalanced, they can be a danger to themselves and those they are trying to help. It can even lead to “compassion fatigue”, where even the most compassionate can “lose sight of their end goals or become cynical and detached”. A need to rethink the humanitarian sector and its actions At the 2016 World Humanitarian Summit, Brendan McDonald, along with other colleagues, attempted to petition the summit, calling on the UN to “prioritise staff well-being”. “I was told by UNOCHA senior management not to pursue the matter; it was basically not seen as an issue.” While this interaction has left McDonald with “zero faith in the system”, Amjad Saleem, manager for the Volunteer section of the IFRC believes this summit was an attempt to rethink the humanitarian sector and its actions and open a dialogue on mental health. For McDonald, working in countries where there is often no rule of law, aid workers struggle to find someone to turn to, and in one of the world’s largest unregulated sectors, “the bullying, the harassment, the poor leadership, the arbitrary dismissal of staff, the inherent racism, misogyny and sexual harassment are very present”. Here at FD Consultants we take this subject seriously and offer support for organisations and individuals both before a humanitarian assignment, during and after. For our full list of services, or to talk to us about how we can support you, or your volunteer staff, click here Hosted by the Mental Health Foundation, Mental Health Awareness Week 2019 will take place from Monday 13 to Sunday 19 May 2019. The theme for 2019 is Body Image – how we think and feel about our bodies. All of us live with our bodies as they evolve and change. Just as all of us have a role in shaping an inclusive culture where we help others feel comfortable in their own skin. Body image and self-esteem start in the mind, not in the mirror. They can change the way you understand your value and worth. Healthy body image and self-esteem are a big part of well-being. Body image is mental and emotional: it’s both the mental picture that you have of your body and the way you feel about your body when you look in a mirror. Healthy body image is more than simply tolerating what you look like or “not disliking” yourself. A healthy body image means that you truly accept and like the way you look right now and aren’t trying to change your body to fit the way you think you should look. It means recognising the individual qualities and strengths that make you feel good about yourself beyond weight, shape or appearance, and resisting the pressure to strive for the myth of the “perfect” body that you see in the media, online, in your communities. Self-esteem is how you value and respect yourself as a person—it is the opinion that you have of yourself inside and out. Self-esteem impacts how you take care of yourself, emotionally, physically, and spiritually. Self-esteem is about your whole self, not just your body. When you have good self-esteem, you value yourself, and you know that you deserve good care and respect—from yourself and from others. You can appreciate and celebrate your strengths and your abilities, and you don’t put yourself down if you make a mistake. Good self-esteem means that you still feel like you’re good enough even when you’re dealing with difficult feelings or situations. Why do body image and self-esteem matter? Body image and self-esteem directly influence each other—and your feelings, thoughts, and behaviours. If you don’t like your body (or a part of your body), it’s hard to feel good about your whole self. The reverse is also true: if you don’t value yourself, it’s hard to notice the good things and give your body the respect it deserves. Below, see how good body image and self-esteem positively impact mental health: 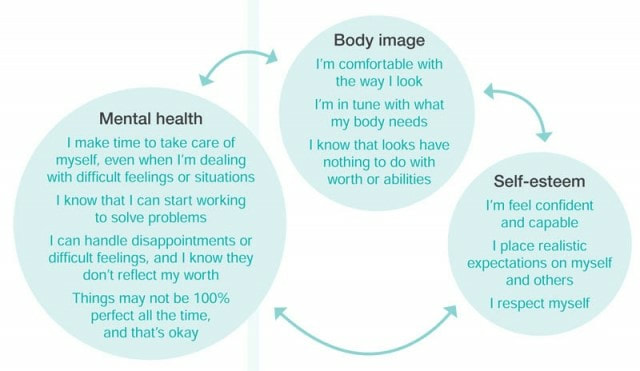 These are just a few examples. As you can see, good body image, self-esteem, and mental health are not about making yourself feel happy all the time. They are about respecting yourself and others, thinking realistically, and taking action to cope with problems or difficulties in healthy ways. Below, see how poor body image and self-esteem negatively impact mental health: 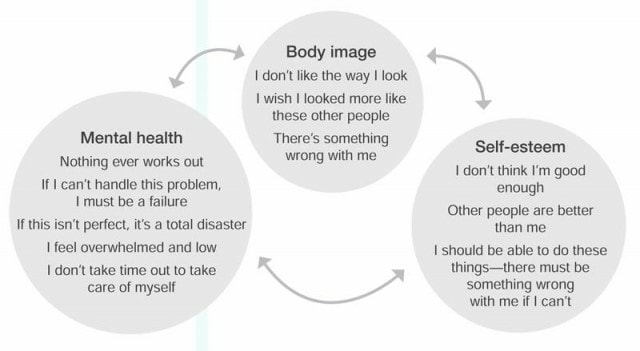 As you can see, the problem with negative thinking and feelings is that once people start to focus on shortcomings or problems in one area or one situation, it becomes very easy to only see problems in many other areas or situations. Negative thinking has a way of leading to more negative thinking.
How can I encourage a healthier body image?
The next time you notice yourself having negative thoughts about your body and appearance, take a minute to think about what’s going on in your life. Are you feeling stressed out, anxious, or low? Are you facing challenges in other parts of your life? When negative thoughts come up, think about what you’d tell a friend if they were in a similar situation and then take your own advice. Be mindful of messages you hear and see in the media and how those messages inform the way people feel about the way they look. Recognise and challenge those stereotypes! |

CONTACTArchives
April 2022
Categories
All
|
 RSS Feed
RSS Feed
